Breast Self-Examination
Breast self-examination is a simple yet meaningful practice of self-observation. Its primary role is not diagnosis, but rather familiarizing the woman with the normal shape and texture of her breasts. Through systematic repetition, a woman gains awareness of what is normal for her own body, so she can promptly recognize any new change.
It is important to clarify that self-examination does not replace clinical evaluation by a specialized physician or imaging studies (mammography or ultrasound). It functions as a complement within an overall strategy of prevention and early detection.
When should it be performed?
The timing of self-examination matters, as hormonal fluctuations during the menstrual cycle affect the texture and sensitivity of the breasts.
In premenopausal women, self-examination is recommended 5-7 days after the onset of menstruation, when the breasts are less swollen and tender.
In postmenopausal women, it is advisable to choose a specific date each month to maintain consistency in monitoring.
A frequency of once per month is sufficient. Excessively frequent palpation does not increase diagnostic accuracy and may cause anxiety or misleading impressions.
How is it performed correctly?
Self-examination includes two distinct stages: visual inspection and palpation.
Visual inspection
The woman stands in front of a mirror in a well-lit area. Observation is performed first with the arms relaxed at the sides, then with the arms raised, and finally with the hands pressed against the hips to contract the chest muscles.
During inspection, breast symmetry is assessed, bearing in mind that mild asymmetries are often normal. Particular attention is given to newly appearing changes, such as nipple retraction, skin thickening or dimpling, redness, edema with a “peau d’orange” appearance, or the presence of nipple discharge.
The goal of observation is to recognize changes compared to the previous appearance, not to seek “perfect symmetry.”
Palpation
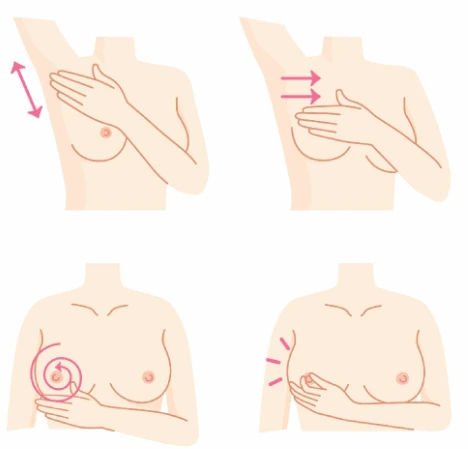
Palpation is performed in the supine position, using the opposite hand from the breast being examined. The pads of the three middle fingers are used, with circular and systematic movements.
Pressure is applied at three levels: light for the superficial tissues, moderate for the intermediate layers, and deeper for examining the chest wall. Systematic coverage is important to ensure the entire breast is examined without missing any area.
Palpation may follow a circular pattern, a radial pattern, or vertical parallel movements (linear scanning). Whichever pattern is chosen, it is important to apply it consistently every month. The examination is completed with an assessment of the axillary area, where the axillary lymph nodes are located.
Which findings should prompt medical evaluation?
Any new palpable lump, change in breast texture, persistent localized tenderness, skin changes, bloody nipple discharge, or swelling in the axilla should be evaluated by a specialist.
It is important to emphasize that the majority of palpable findings, especially in younger women, are benign. Seeking medical evaluation does not automatically mean a serious diagnosis; rather, it represents a responsible attitude toward one’s health.
The realistic role of self-examination
In the current medical literature, self-examination is not considered an independent screening method. However, it remains valuable as a tool for empowerment and body awareness. A woman who knows her body is more likely to recognize a change early and seek medical advice.
Self-examination should not create anxiety or replace organized preventive screening. Instead, it is part of an overall culture of prevention, based on knowledge, consistency, and collaboration with a specialized physician.
Guidance and education
Breast self-examination is a simple procedure; however, many women are uncertain whether they perform it correctly. It is entirely normal to have questions or feel unsure about what exactly should be palpated and how a finding should be assessed.
During your visit to the office, time is dedicated to practical guidance, if you wish. Through individualized instructions, you can learn the correct palpation technique, understand the normal texture of your own breast, and become familiar with what is expected and what requires further evaluation.
Knowledge and understanding reduce anxiety and boost confidence. Self-examination is not a test driven by “fear” but a form of caring for your body.
Prevention is most effective when it is based on knowledge and collaboration.
What is considered a suspicious finding?
The majority of palpable lesions are benign. However, medical evaluation is required when the following are observed:
- a new palpable mass that persists,
- a hard area with ill-defined borders,
- a change in the shape or size of the breast,
- new-onset nipple retraction,
- bloody discharge,
- persistent unilateral breast pain accompanied by a finding.
Any new or changing finding that persists beyond one menstrual cycle should be clinically evaluated.
What every woman should know
Breasts normally have a heterogeneous texture. The presence of areas with increased density or fibrocystic tissue is a common and benign finding, particularly in women of reproductive age. The sensation of “graininess,” small nodules, or alternating firmer and softer areas is often related to hormonal fluctuations and does not necessarily indicate pathology.
Self-examination has not been shown to independently reduce breast cancer mortality, according to international literature data. However, it retains an important role as a tool for body awareness. A woman who knows the normal anatomy of her breasts is better able to recognize a new or changing lesion early and to seek medical evaluation without delay.
Proper education reduces unwarranted panic, prevents excessive worry over normal findings, and fosters a mature and responsible attitude toward health.
Self-examination is part of a comprehensive prevention strategy that includes regular clinical examination by a specialized physician, imaging surveillance according to age and individual risk profile, and personalized medical follow-up.
Prevention is not based on fragmented practices but on consistency, scientific evidence, and physician-patient collaboration. Knowledge and consistency are the most powerful tools for early diagnosis — not fear.